Maternity Telemedicine Services in the Aegean Islands
M. Gatzonis *, S. Deftereos, MD *, P. Vasiliou, MD +, F. Dimitriou, Midwife $, G. Creatsas, Prof., MD^, D. Sotiriou *, Assoc. Prof.*, K. Boddy, Senior Lecturer, MD %
(paper presented by M. Gatzonis, in the 2nd International Conference on Telemedicine, Toulouse, March 22-24, 2000)
* Medical Physics Laboratory, School of Medicine, University of Athens, Greece
+ Healthcare Centre of Naxos, Greece
$ Healthcare Centre of Mykonos, Greece
^ Aretaieion Hospital, Greece
% Royal Infirmary of Edinburgh, UK
ABSTRACT
HERMES (Telematic Healthcare Remoteness And Mobility Factors In Common European Scenarios), a 4th Framework Programme Project of the Commission of the European Union, designed a platform for the development of quality assured Telemedicine Services at the point of need. In the context of the platform’s evaluation, the HERMES Greek partners have implemented Maternity Telemedicine Services between the Primary Healthcare Centres of the Islands of Naxos and Mykonos, in the region of the Aegean Sea, and the Aretaieion University Hospital in Athens, Greece. The services are offered by expert gynaecologists / obstetricians to primary care physicians and/or midwives, confronted with emergency or difficult to interpret maternity cases. Patient related information is recorded with the aid of patient record software, and may include (textual) gynaecological information and Cardiotocograms (CTGs). The records are transmitted to experts via ISDN links, while discussion on the case can be performed via video-conferencing. During the initial implementation phase, the maternity services have been offered to 40 individuals. The services are found to be a significant aid for Primary Care Units that do not have access to obstetric expertise.
INTRODUCTION
HERMES (Telematic Healthcare Remoteness And Mobility Factors In Common European Scenarios) a 4th Framework Programme Project of the Commission of the European Union, designed a platform for the development of quality assured Telemedicine Services at the point of need. In the context of the platform’s evaluation, the HERMES consortium has implemented Maternity Telemedicine Services between the Primary Healthcare Centres of the Islands of Naxos and Mykonos, in the region of the Aegean Sea, and the Aretaieion University Hospital in Athens, Greece.
Maternity services are of major importance for the Aegean Islands, mainly due to their isolation, especially during winter. Traditionally, maternity services in Naxos and Mykonos are offered by the Healthcare Centres of those islands, as well as by obstetricians working in private practices. Healthcare Centres in both Naxos and Mykonos are manned by Internists, General Practitioners and young, non-specialised physicians. The lack of gynaecologists / obstetricians together with the limited experience of the serving staff on obstetric issues, pose difficulties in the routine follow-up of pregnant women and in the handling of emergency cases. Private practices, on the other hand, are usually not adequately equipped to handle difficult or emergency cases.
As a consequence, pregnant women choose to take their follow up examinations at tertiary hospitals in Athens. Furthermore, they prefer private over public maternity hospitals. During their pregnancy they have to travel to Athens as many as 10 times. Travel costs, including clinic fees, hotel staying and travel expenses, are (in the majority of cases) undertaken by the ladies themselves. Emergency cases are evacuated to tertiary hospitals either by boat or aeroplane, depending on the severity of the case and on weather conditions. It is a rather common situation that during winter, travelling by boat or even by plane is often impossible due to adverse weather conditions for as long as one week.
In order to assist primary care physicians to better handle difficult to diagnose and/or emergency maternity cases, and in providing quality routine follow up services to the local populations, we have introduced Maternity Telemedicine Services between primary healthcare units supported by a tertiary Obstetrics and Gynaecology Clinic.
SERVICE DESIGN AND IMPLEMENTATION
Maternity Telemedicine Services have been designed according to the HERMES 7-step methodology [2]. All user categories (physicians, midwives, technicians, representatives of the local community) involved have played an active role during the entire design process. User views have been systematically gathered with the aid of a specialized tool, the HERMES Question Set [4]. The services have been modelled according to the services provided in the Lothian Region of Scotland, by the Royal Infirmary of Edinburgh[1].
Physicians and midwifes have studied the Guidelines for Antenatal Care [3] in use at the Edinburgh region and have agreed that they can be used in Greece as well.
Routine examinations of pregnant ladies are based on physical examinations such as blood pressure recordings, urine analysis and measurement of the uterine size. The wellbeing of the baby is assessed using fetal movements (‘kicks’) as well as recordings of the foetal heart rate, obtained using a cardiotocograph. Cardiotocograms are easy to acquire in every day practice and they pose no threats to the health of either the mother or the foetus. They provide important information on the dynamic condition of the foetus.
Hardware and software
The hardware and software infrastructure of the participating sites includes a Intel Pentium based PC, equipped with 32MB of RAM, running Microsoft’s Windows NT Workstation or Windows 98. The PC is able to participate in a point-to-point videoconference session using Intel’s Business Conferencing System. The ISDN adapter of the Conferencing system is also used to establish a ISDN (TCP/IP) link between the participating sites for the transmission of a patient’s Electronic Record. The link was established through the ISDN router (CISCO 1604) of the Medical Physics Laboratory.
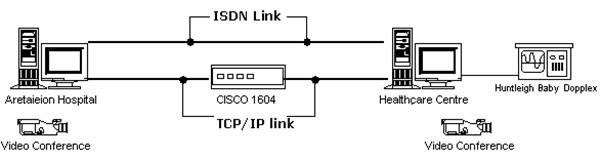
In this study the CTGs’ were acquired using the Huntleigh Baby Dopplex [5] digital cardiotocograph and were recorded in a database using the Oxford Instruments Teamview software [6]. Teamview Software was also installed at the supporting hospital and was used as a viewer for the transmitted CTGs’.
The Teamview Software and web-based viewer is composed of four parts:
-
Administration: physicians and/or midwives use this module to create patient Electronic Records. Basic administrative data (name, date of birth, expected date of delivery) was recorded and all patient data including the CTG traces were stored in a relational database, typically based on Microsoft’s Accessâ.

Main selection screen (view/create patient records)
-
CTG Traces: the module is used to acquire, view and annotate CTG traces. Traces are displayed synchronously to their acquisition. The usual recording time of a CTG is 20 minutes.
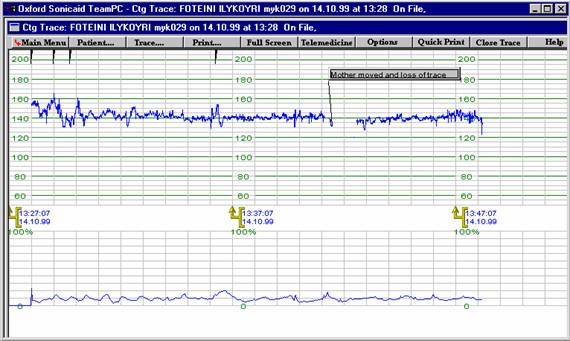
CTG trace Window Recording/Viewing a CTG trace
-
Dialog boxes where physicians or midwifes can describe questions to the experts: Using the same dialog boxes the experts at the supporting hospital can record their opinion, which can be viewed later by the remote physicians.
-
A Telematic module for transmission: with a click of a button the Electronic Patient Record (EPR) can be transmitted to and stored in the ‘medical server’, which is situated at the Medical Physics Laboratory of the University of Athens. From the medical server, data can also be retrieved and updated by the supporting hospital. The medical server is based on Microsoft’s SQL Server, installed on Intel’s Pentium Workstation running Windows NT Server.
Telemedicine Sessions
Telemedicine
Services are initiated by primary care physicians’ and/or midwives, when they
are confronted with an emergency maternity case, or they are in need of expert
advice on a routine follow up examination of a pregnant woman. Telemedicine
sessions are initiated with patient consent and they typically include:
-
Creation (or update) of the patient’s Electronic Patient Record (EPR)
-
Recording of the cardiotocogram (CTG) trace and insertion in the record
-
Transmission of the EPR to the medical server hosted at the Medical Physics Laboratory (School of Medicine, University of Athens)
-
Alert of the physicians of the 2nd Obstetrics and Gynaecology Department of the Aretaieion University Hospital in Athens via e-mail, telephone or video conference
-
Review of the EPR of the patient by expert physicians, recording of their opinion and storage of the added information to the server archives
-
Discussion of the case between hospital experts and remote physician and/or midwifes, via telephone or video-conference (depending on the case) if need arises
-
Handling the case at remote site as agreed
RESULTS AND DISCUSSION
During the initial implementation phase, both technical and clinical aspects of the service have been evaluated. Evaluation of the Electronic Healthcare Record, video-conferencing and CTG recording and processing modules focused on their reliability, user-friendliness and availability. Network evaluation focused on its reliability, availability and speed, expressed in terms of the time required to perform key operations. Clinical evaluation focused on the adequacy of the communicated information for reaching a decision when distance separates patient and expert physician.
During the period being reported (August 1998 – February 2000) thirty Telemedicine sessions have taken place between the Healthcare Centre of Mykonos and the 2nd Obstetrics and Gynaecology Clinic, while ten sessions were originated from the Healthcare Centre of Naxos.
In all cases a single attempt sufficed to establish the Telemedicine link. The time required to transfer patient EHCRs between the primary and tertiary sites was always less than 15 seconds. Communication problems were not encountered during the entire period.
Video conferencing links were established after EHCR data had been transfered, to allow communication between the consulting and the primary care physicians and/or midwives requesting assistance. The links were again easily established, remained active during the entire consultations and were found to be of good quality for the purposes of the service.
The Electronic Patient Record and the CTG recording and processing modules were found to be reliable, as no problems were encountered. Their availability was expected to be high by design, which proved to be true. The availability and reliability of the server on which the patient EPRs are stored, at the Medical Physics Laboratory, were also found to be high.
The use of all modules proved to be easy. Participating medical professionals felt comfortable with the software after a short training period of about one day. The average time required to study and update an existing patient EPR was approximately five (5) minutes, while the time required to create a new EPR was 10 minutes. The time required to record a CTG trace and to attach it to the patient record was around 25 minutes. This is in accord with the Maternity Guideline, which states that each recording should be of at least 20 minutes duration. The overall time required to record patient data for the first time was, therefore, less than 35 minutes, which was considered acceptable.
Maternity Telemedicine services were offered in 40 cases. All cases, concerned pregnant women taking routine follow-up examinations. All cases but one were found to be normal. Only one of the patients presented with a complicated clinical condition, namely that of premature labour associated with placenta praevia. Primary care physicians, following the advice obtained using the telemedicine system, evacuated the patient to the Aretaieion hospital. Overall in this study, the contents of the patient EPR, including the CTG trace, proved to be adequate in reaching a safe decision for all 40 cases.
Maternity Telemedicine services were found to be a significant aid to Primary Care Units that do not have access to specialised obstetric expertise. By providing healthcare employees of those units with easy, on-demand access to expert advice, they improve the quality of the services provided to pregnant ladies; they allow an optimal selection of cases that are in need of evacuation to tertiary units, which, together with improving the quality of locally offered routine follow-up examination, may lead to a substantial reduction of costs and patient satisfaction. As a result, patient displacement can be reduced to a minimum for routine examinations. Due to the big number of pregnancies pen anum in the two islands (50 in average), this leads to a considerable reduction of mobility costs. The return on the investment of the telematic infrastructure and the medical devices can thus be achieved in a little more than a year.
NEW DEVELOPMENTS
Despite the fact that the content of patient records, including CTGs, were found to be sufficient for treating maternity cases, it was generally recognised that a more generic customisation of the EPR software would increase the richness of information it contains and would facilitate experts in gaining a better understanding of the cases being handled. Information provided orally (e.g. via video-conference) and not stored in patients’ records increase the length of Telemedicine sessions and increase the risk of loosing or misinterpreting the data.
The Medical Physics Laboratory of the University of Athens in collaboration with the participating sites has now developed a sophisticated, web-based, Electronic Healthcare Record Software (EHCRS), which addresses the above mentioned requirements. The software is currently being tested and it should be installed at the participating sites within the next few months. In addition to CTG traces, EHCRS allows patient records to contain all information required to establish a diagnosis for a presenting complaint and to decide on required follow-up actions. Examples of such information are: the complete medical history of the patient with emphasis on important obstetric and gynaecological data, ultrasound data, the results of previous physical examinations and the results of laboratory and other investigations undertaken in the past.
Further more, the UOA Medical Physics Laboratory is testing the possibility of transferring, in real-time, ultrasound video signals, by using the videoconferencing equipment. Initial tests have been successful. The supporting hospital will decide whether the quality of the transmitted data is adequate for diagnostic purposes.
In addition to improving technical and functional aspects of maternity services in the Aegean region, future work will focus on their more rigorous evaluation. The initial results, however, are encouraging.
REFERENCES
[1] Saling E., Comments on past and present situation of intensive monitoring of the fetus during labor, J Perinat Med, 1996, 24:1, 7-13
[2] The HERMES 7 Step Methodology, HERMES Deliverable 9.3, ‘Functional Specifications and Report on HERMES Future Work / Business Plans, for Harmonisation. Demonstration and Uptake of ‘A Global 24 Hours TMS Platform of Urgent Response Services Delivered to the Point of Need’’, January 1999
[3] K. Boddy et al., Guidelines for Antenatal Care, Royal Infirmary of Edinburgh, December 1986. Information can also be obtained for the electronic pages at http://www.telemedicine.ed.ac.uk/maternity/default.htm
[4] Huntleigh Diagnostics, UK (Fetal Monitoring Equipment producer)
[5] The HERMES Question Set, HERMES Deliverable 2.1 ‘Pilot Site Analysis of User Requirements including Functional Marketing Specification and Electronic Service Description Tool’, August 1996
[6] K. Boddy, P. Karpp, D. Sotiriou, ‘Telemedicine and Telecare for the New Information Age’, Financial Times Report, November 26, 1999
Additional References
D G Moris, Using telemedicine to facilitate training in cardiotocography (CTG) interpretation, Journal of Telemedicine and Telecare 2000;6 (suppl. 1): 53-5
Andrew Dawson, David Cohen, Claire Candelier, Gill Jones, Julia Sanders, Andy Thompson, Cliff Arnall, Edward Coles. Domiciliary midwifery support in high-risk
Pregnancy incorporating telephonic fetal heart rate monitoring: a health technology randomized assessment. Journal of Telemedicine and Telecare 1999;5:220-230
Tõrõk M, Turi Zs, Kovács F. Ten years’ clinical experience with telemedicine in prenatal care in Hungary. Journal of Telemedicine and Telecare 1999;5 (suppl. 1):14-17
Dawson AJ, Middlemiss C, Coles E, Gough N, Jones E. A randomized study of a domiciliary antenatal care scheme: the effect on hospital admissions. British Journal of Obstetrics and Gynaecology 1989;96:1319-22
Fisk NM, Sepulveda W, Drysdale K, et al. Fetal telemedicine: six month pilot of real-time ultrasound and video consultation between the Isle of Wight and London. British Journal of Obstetrics and Gynaecology 1996;103:1092-5
House of Common Health Select Committee (chairman Winterton N). Second Report: Maternity Services, Volume 1. London: HMSO, 1992
Wyatt J. Evaluating the impact of telemedicine on health professionals and patients. In: Rigby M, ed. Taking Health Telematics Safely into the Twenty-First Century. Oxford: Radcliffe Medical Press (In press)
Klutke PJ, Mattioli P, Baruffaldi F. Fifty-seven rules for effective video Conferencing in telemedicine. http://www.tecno.ior.it/telemed/Projects/phnet/index.html, link to the file MPVCRule.doc